
STRUCTURE OF INJURIES AMONG MILITARY PERSONNEL CAUSED BY THE USE OF ENEMY FPV (FIRST-PERSON VIEW) DRONES
- Apr 21
- 4 min read
Mykhailo NIKOLAIEV, PhD
Head of the Forward Surgical Team, Zaporizhzhia Military Hospital, Zaporizhzhia, Ukraine.
Roman KUZIV
Lieutenant Colonel of the Medical Service
Commander of the Military Medical Clinical Center of the Eastern Region
Introduction
In the russo-Ukrainian war, the use of FPV (First-Person View) drones has gained significant importance for both sides of the conflict. These drones are employed for both reconnaissance and strike missions and have become an integral part of emerging tactics on the modern battlefield. The role of FPV drones has increased particularly due to the complexity of combat in environments where traditional methods are limited, while direct target control enhances the probability of a successful hit.
The use of modified commercial drones, such as the Mavic platform, for deploying grenades or other explosive devices has also become a widespread practice in combat operations.
An analysis was conducted of injuries in 692 military personnel caused by the use of enemy FPV (First-Person View) drones in the Zaporizhzhia operational direction among combat units during the period from 01 January 2026 to 01 February 2026, accounting for 64.55% of the total number of wounded.
The following parameters were identified:
• Predominant injury locations
• Combined injuries (involvement of two anatomical regions)
• Injuries involving more than three anatomical regions
• Incidence of burns among the total number of wounded
• Incidence and distribution of blast-related injuries (barotrauma)
• Incidence of poisoning by chemical warfare agents

Dominant | Cases | % |
Head and neck injuries | 279 | 40,32 |
Chest and back injuries | 60 | 8,67 |
Abdominal and lumbar injuries | 28 | 4,05 |
Pelvic and gluteal injuries | 23 | 3,32 |
Spinal injuries | 1 | 0,14 |
Upper extremity injuries | 126 | 18,21 |
Lower extremity injuries | 161 | 23,27 |
Soft tissue injuries | 13 | 1,88 |
Poisoning | 1 | 0,14 |
Total FPV-related injuries | 692 | 100 |
% of total injuries | 64,55 |
The total number of wounded with injuries affecting two anatomical regions was 380 (54.91%).
The total number of wounded with injuries affecting three or more anatomical regions was 142 (20.52%).

Combined | Cases | % |
Single anatomical region involved | 312 | 45,09 |
Upper extremity injuries | 137 | 19,8 |
Lower extremity injuries | 100 | 14,45 |
Head and neck injuries | 53 | 7,66 |
Chest and back injuries | 41 | 5,92 |
Abdominal and lumbar injuries | 24 | 3,47 |
Pelvic and gluteal injuries | 22 | 3,18 |
Soft tissue injuries | 2 | 0,29 |
Spinal injuries | 1 | 0,14 |
Poisoning | 0 | 0 |
Total | 692 | 100 |

More than two anatomical regions | Cases | % |
Injuries involving only two anatomical regions | 238 | 34,39 |
Single anatomical region involved | 312 | 45,09 |
Lower extremity injuries | 88 | 12,72 |
Upper extremity injuries | 20 | 2,89 |
Head and neck injuries | 14 | 2,02 |
Abdominal and lumbar injuries | 7 | 1,01 |
Pelvic and gluteal injuries | 7 | 1,01 |
Chest and back injuries | 6 | 0,87 |
Spinal injuries | 0 | 0 |
Soft tissue injuries | 0 | 0 |
Poisoning | 0 | 0 |
Total | 692 | 100 |
Number of wounded with burns among the total number of injuries:
Cases | % | |
Burns | 36 | 5,2 |

Blast-related injuries (barotrauma) among the total number of FPV casualties:
Blast-related injury (barotrauma) | Cases | % |
With tympanic membrane perforation | 52 | 7,5 |
Without perforation / tinnitus | 244 | 35,3 |
Total | 296 | 42,8 |

Of these, the number of wounded admitted with tourniquet syndrome:
Cases | % | |
Tourniquet-associated limb syndrome | 13 | 1,88 |

Tourniquet-associated syndrome is a pathological condition resulting from prolonged compression of a limb by a tourniquet, leading to impaired blood circulation. The syndrome develops due to extended tourniquet application.
Main consequences of tourniquet-associated syndrome:
Tissue ischemia
Muscle necrosis and damage
Plegia and paresthesia
Acute kidney injury following tourniquet release from an ischemic limb
CWAs (chemical warfare agents)
Poisoning | Cases | % |
Poisoning | 2 | 0,29 |

Unmanned aerial vehicles are used to deploy containers with toxic agents, likely chloropicrin-based K-51 grenades.
Distribution by severity:
Cases | % | |
Mild | 515 | 74,42 |
Moderate | 109 | 15,75 |
Severe (requiring intensive care) | 68 | 9,83 |
Total | 692 | 100 |
Distribution by evacuation time (hours):
Hours | Cases | % |
<1 | 33 | 4,77 |
1-3 | 153 | 22,11 |
3-6 | 99 | 14,31 |
6-12 | 95 | 13,73 |
12-24 | 81 | 11,71 |
24-48 | 86 | 12,43 |
48-72 | 39 | 5,64 |
>72 | 106 | 15,32 |
Total | 692 | 100 |
average evacuation time to Role 2 | 44 hours |
!!! Content Warning !!!
The following content may contain descriptions of traumatic injuries, medical procedures, or battlefield-related events that may be disturbing or sensitive for some viewers. Viewer discretion is advised.
Examples of head injuries






Examples of abdominal injuries







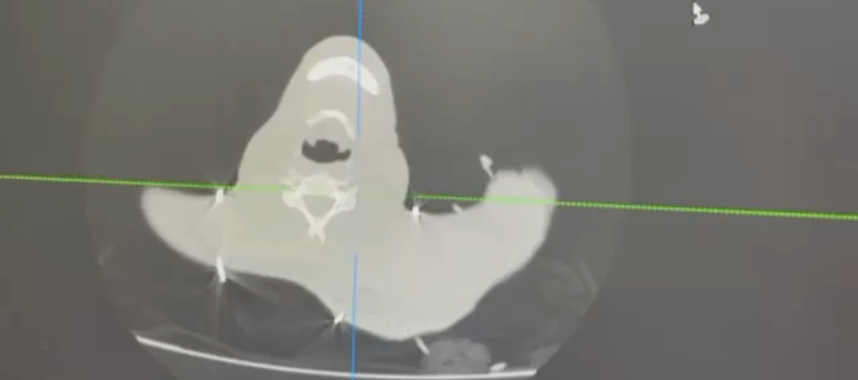



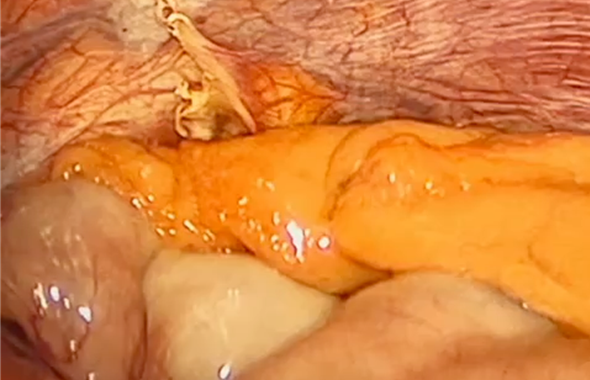
Examples of limb injuries (vascular injuries)






Examples of extremity injuries












Summary
Head and neck injuries are the most frequent, accounting for 40.32% of all cases. The total number of blast-related injuries (barotrauma) is 296 cases (42.8%) of the overall total. This indicates the vulnerability of these regions despite the use of protective helmets and highlights the need for active tactical hearing protection.
Extremity injuries also represent a significant issue, with lower extremity injuries accounting for 23.27% and upper extremity injuries for 18.21%, demonstrating the relative lack of protection of these areas. These injuries reduce mobility and combat effectiveness.
Combined extremity injuries: Together, upper and lower extremity injuries account for over 41% of predominant injuries and more than 34% of combined injuries. This underscores the need for a sufficient supply of hemorrhage control devices (tourniquets) and external fixation systems.
Multiple injuries: Every fifth wounded individual (20.52%) has injuries involving more than two anatomical regions, which significantly complicates stabilization and requires multidisciplinary surgical teams.
Lower-priority categories: Poisoning and isolated spinal injuries account for the smallest proportion, approximately 0.14%.
Proposals for Improving the Protection of Military Personnel:
1.Enhanced head and neck protection:
Use of helmets that provide extended coverage of the face, neck, and occipital region.
Incorporation of additional neck protection elements (e.g., ballistic neck collars) to reduce the risk of injury to this area.
Extremity protection:
Use of lightweight Kevlar-based materials that do not restrict mobility while providing protection against small fragments.
Pelvic and gluteal protection:
Use of groin protection modules (ballistic inserts), as injuries to these regions are often severe.
2.Modernization of body armor and protective materials for the torso:
Improvement of body armor systems with additional lateral ballistic protection (Gen2) for the chest, back, and abdomen, as the torso accounts for approximately 36% of total body surface area and remains at high risk of injury.
Regular training in the proper use of protective equipment to maximize its effectiveness, along with consistent monitoring of compliance among military personnel.
Comments